La Gran Bretagna avvia la maxi campagna vaccinale contro Covid-19, ma non per tutti. Il vaccino di Pfizer, come stabilito in un documento della Joint Committee on Vaccination and Immunisation, non sarà iniettato a donne incinte, che allattano e a chi ha intenzione di avere una gravidanza.
VIA ALLA VACCINAZIONE
Nei giorni scorsi il Regno Unito ha concesso l’autorizzazione di emergenza al vaccino anti Covid di Pfizer. È il primo Paese occidentale a consentire vaccinazioni di massa contro Covid-19, anticipando anche gli Usa.
ESCLUSE DONNE INCINTE
Escluse dalla vaccinazione, almeno al momento, saranno le donne incinte, chi desidera una gravidanza a breve e i lattanti.
“I dati sull’uso del vaccino mRna Covid-19 Bnt162b2 non esistono o sono limitati. Gli studi di tossicità riproduttiva sugli animali non sono stati completati”, spiega l’Autorità. E per questo il “Vaccino mRna Covid-19 Bnt162b2 non è raccomandato durante la gravidanza”.
Alle “donne in età fertile deve essere consigliato di evitare la gravidanza per almeno 2 mesi dopo la seconda dose”.
IMPATTO SULLA FERTILITA’?
Non solo. Il vaccino potrebbe avere anche un impatto sulla fertilità e quindi, al momento, è sconsigliato a chi desidera un vaccino.
QUANDO NO AL VACCINO PFIZER
No al vaccino anche per le donne che allattano. “Non è noto se il vaccino COVID-19 mRna Bnt162b2 sia escreto nel latte umano”, scrive l’Autorità. Il vaccino sarebbe “un rischio per i neonati/bambini”.
+++
+++
Qui il documento completo del Joint Committee on Vaccination and Immunisation
REG 174 INFORMATION FOR UK HEALTHCARE PROFESSIONALS
This medicinal product does not have a UK marketing authorisation but has been given authorisation for temporary supply by the UK Department of Health and Social Care and the Medicines & Healthcare products Regulatory Agency for active immunization to prevent COVID-19 disease caused by SARS-CoV-2 virus in individuals aged 16 years of age and over.
As with any new medicine in the UK, this product will be closely monitored to allow quick identification of new safety information. Healthcare professionals are asked to report any suspected adverse reactions. See section 4.8 for how to report adverse reactions.
1. NAME OF THE MEDICINAL PRODUCT
COVID-19 mRNA Vaccine BNT162b2 concentrate for solution for injection
2. QUALITATIVE AND QUANTITATIVE COMPOSITION
This is a multidose vial and must be diluted before use. 1 vial (0.45 mL) contains 5 doses of 30 micrograms of BNT162b2 RNA (embedded in lipid nanoparticles).
COVID-19 mRNA Vaccine BNT162b2 is highly purified single-stranded, 5’-capped messenger RNA (mRNA) produced by cell-free in vitro transcription from the corresponding DNA templates, encoding the viral spike (S) protein of SARS-CoV-2.
Excipients with known effect:
For the full list of excipients, see section 6.1.
3. PHARMACEUTICAL FORM
Concentrate for solution for injection.
The vaccine is a white to off-white frozen solution.
4. CLINICAL PARTICULARS
4.1 Therapeutic indications
Active immunisation to prevent COVID-19 caused by SARS-CoV-2 virus, in individuals 16 years of age and older.
The use of COVID-19 mRNA Vaccine BNT162b2 should be in accordance with official guidance.
4.2 Posology and method of administration
Posology
Individuals 16 years of age and older
COVID-19 mRNA Vaccine BNT162b2 is administered intramuscularly after dilution as a series of two doses (0.3 mL each) 21 days apart (see section 5.1). There are no data available on the interchangeability of COVID-19 mRNA Vaccine BNT162b2 with other COVID-19 vaccines to complete the vaccination series. Individuals who have received one dose of COVID-19 mRNA Vaccine BNT162b2 should receive a second dose of COVID-19 mRNA Vaccine BNT162b2 to complete the vaccination series.
Individuals may not be protected until at least 7 days after their second dose of the vaccine.
For further information on efficacy, see section 5.1.
Paediatric population
The safety and efficacy of COVID-19 mRNA Vaccine BNT162b2 in children under 16 years of age have not yet been established.
Method of administration
Administer the COVID-19 mRNA Vaccine BNT162b2 vaccine intramuscularly in the deltoid muscle after dilution.
Do not inject the vaccine intravascularly, subcutaneously or intradermally.
Preparation: The multidose vial is stored frozen and must be thawed prior to dilution.
For instructions on disposal see section 6.6.
4.3 Contraindications
Hypersensitivity to the active substance or to any of the excipients listed in section 6.1.
4.4 Special warnings and precautions for use
Traceability
In order to improve the traceability of biological medicinal products, the name and the batch number of the administered product should be clearly recorded.
General recommendations
As with all injectable vaccines, appropriate medical treatment and supervision should always be readily available in case of a rare anaphylactic event following the administration of the vaccine.
The administration of COVID-19 mRNA Vaccine BNT162b2 should be postponed in individuals suffering from acute severe febrile illness.
Individuals receiving anticoagulant therapy or those with a bleeding disorder that would contraindicate intramuscular injection, should not be given the vaccine unless the potential benefit clearly outweighs the risk of administration.
Immunocompromised persons, including individuals receiving immunosuppressant therapy, may have a diminished immune response to the vaccine. No data are available about concomitant use of immunosuppressants.
As with any vaccine, vaccination with COVID-19 mRNA Vaccine BNT162b2 may not protect all vaccine recipients.
No data are available on the use of COVID-19 mRNA Vaccine BNT162b2 in persons that have previously received a full or partial vaccine series with another COVID-19 vaccine.
Excipient information
This vaccine contains potassium, less than 1 mmol (39 mg) per dose, i.e. essentially ‘potassium-free’.
This vaccine contains less than 1 mmol sodium (23 mg) per dose, i.e. essentially ‘sodium‑free’.
4.5 Interaction with other medicinal products and other forms of interaction
No interaction studies have been performed.
Concomitant administration of COVID-19 mRNA Vaccine BNT162b2 with other vaccines has not been studied (see section 5.1).
Do not mix COVID-19 mRNA Vaccine BNT162b2 with other vaccines/products in the same syringe.
4.6 Fertility, pregnancy and lactation
Pregnancy
There are no or limited amount of data from the use of COVID-19 mRNA Vaccine BNT162b2. Animal reproductive toxicity studies have not been completed. COVID-19 mRNA Vaccine BNT162b2 is not recommended during pregnancy. For women of childbearing age, pregnancy should be excluded before vaccination. In addition, women of childbearing age should be advised to avoid pregnancy for at least 2 months after their second dose.
Breast-feeding
It is unknown whether COVID-19 mRNA Vaccine BNT162b2 is excreted in human milk. A risk to the newborns/infants cannot be excluded. COVID-19 mRNA Vaccine BNT162b2 should not be used during breast-feeding.
Fertility It is unknown whether COVID-19 mRNA Vaccine BNT162b2 has an impact on fertility.
4.7 Effects on ability to drive and use machines
COVID-19 mRNA Vaccine BNT162b2 has no or negligible influence on the ability to drive and use machines. However, some of the adverse reactions mentioned under section 4.8 may temporarily affect the ability to drive or use machines.
4.8 Undesirable effects
Summary of safety profile
The safety of COVID-19 mRNA Vaccine BNT162b2 was evaluated in participants 16 years of age and older in two clinical studies conducted in the United States, Europe, Turkey, South Africa, and South America. Study BNT162-01 (Study 1) enrolled 60 participants, 18 through 55 years of age.
Study C4591001 (Study 2) enrolled approximately 44,000 participants, 12 years of age or older.
In Study 2, a total of 21,720 participants 16 years of age or older received at least one dose of COVID-19 mRNA Vaccine BNT162b and 21,728 participants 16 years of age or older received placebo. Out of these, at the time of the analysis, 19,067 (9531 COVID-19 mRNA Vaccine BNT162b2 and 9536 placebo) were evaluated for safety 2 months after the second dose of COVID-19 mRNA Vaccine BNT162b2.
Demographic characteristics were generally similar with regard to age, gender, race and ethnicity among participants who received COVID-19 mRNA Vaccine and those who received placebo.
Overall, among the participants who received COVID-19 mRNA Vaccine BNT162b2, 51.5% were male and 48.5% were female, 82.1% were White, 9.6% were Black or African American, 26.1% were Hispanic/Latino, 4.3% were Asian and 0.7% were Native American/Alaskan native.
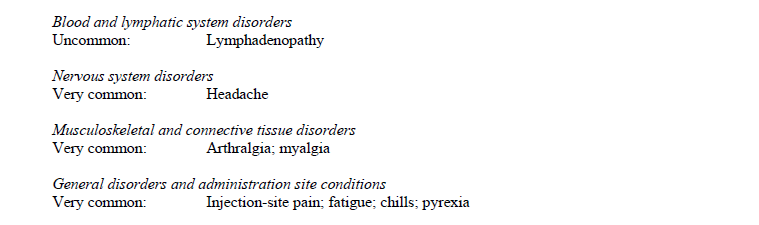
The most frequent adverse reactions in participants 16 years of age and older were pain at the injection site (> 80%), fatigue (> 60%), headache (> 50%), myalgia (> 30%), chills (> 30%), arthralgia (> 20%) and pyrexia (> 10%) and were usually mild or moderate in intensity and resolved within a few days after vaccination. If required, symptomatic treatment with analgesic and/or anti-pyretic medicinal
products (e.g. paracetamol-containing products) may be used.
Adverse reactions from clinical studies
Adverse reactions reported in clinical studies are listed in this section per MedDRA system organ class, in decreasing order of frequency and seriousness. The frequency is defined as follows: very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1,000 to < 1/100), rare (≥ 1/10,000 to < 1/1,000), very rare (< 1/10,000), not known (cannot be estimated from available data).

Reporting of suspected adverse reactions
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the Coronavirus Yellow Card reporting site https://coronavirus-yellowcard.mhra.gov.uk/ or search for MHRA Yellow Card in the Google Play or Apple App Store and include the vaccine brand and batch/Lot number if available.
4.9 Overdose
Participants who received 58 micrograms of COVID-19 mRNA Vaccine in clinical trials did not report an increase in reactogenicity or adverse events.
In the event of overdose, monitoring of vital functions and possible symptomatic treatment is recommended.
5. PHARMACODYNAMIC PROPERTIES
5.1 Pharmacodynamic properties
Pharmacotherapeutic group: {group}, ATC code: not yet assigned Mechanism of action
The nucleoside-modified messenger RNA in COVID-19 mRNA Vaccine BNT162b2 is formulated in lipid nanoparticles, which enable delivery of the RNA into host cells to allow expression of the SARSCoV-2 S antigen. The vaccine elicits both neutralizing antibody and cellular immune responses to the spike (S) antigen, which may contribute to protection against COVID-19 disease.
Efficacy in participants 16 years of age and older
The efficacy of COVID-19 mRNA Vaccine BNT162b2 was evaluated in participants 16 years of age and older in two clinical studies conducted in the United States, Europe, Turkey, South Africa and South America. Study 1 enrolled 60 participants, 18 through 55 years of age. Study 2 is a multicentre, placebo-controlled efficacy study in participants 12 years of age and older. Randomisation was stratified by age: 12 through 15 years of age, 16 through 55 years of age, or 56 years of age and older, with a minimum of 40% of participants in the ≥ 56-year stratum. The study excluded participants who were immunocompromised and those who had previous clinical or microbiological diagnosis of COVID-19 disease. Participants with pre-existing stable disease, defined as disease not requiring significant change in therapy or hospitalization for worsening disease during the 6 weeks before enrolment, were included as were participants with known stable infection with human immunodeficiency virus (HIV), hepatitis C virus (HCV) or hepatitis B virus (HBV). There was no requirement for prophylactic use of paracetamol or analgesics. Influenza vaccines could be administered outside a window ± 14 days of the vaccine doses.
In Study 2, approximately 44,000 participants 12 years of age and older were randomised equally and received 2 doses of COVID-19 mRNA Vaccine or placebo with a planned interval of 21 days. The efficacy analyses included participants that received their second vaccination within 19 to 42 days after their first vaccination. Participants are planned to be followed for up to 24 months, for assessments of safety and efficacy against COVID-19 disease.
The population for the analysis of the primary efficacy endpoint included, 36,621 participants 12 years of age and older (18,242 in the COVID-19 mRNA Vaccine group and 18,379 in the placebo group) who did not have evidence of prior infection with SARS-CoV-2 through 7 days after the second dose.
Demographic characteristics were generally similar with regard to age, gender, race and ethnicity among participants who received COVID-19 mRNA BNT162b2 vaccine and those who received placebo. Overall, among the participants who received COVID-19 mRNA vaccine, 51.1% were male and 48.9% were female, 82.8% were White, 8.9% were Black or African American, 26.8% were Hispanic/Latino, 4.5% were Asian and 0.6% were Native American/Alaskan native. 57.2% were aged 16-55 years, 42.6% were aged > 55 years and 21.8% were ≥ 65 years.
Efficacy against COVID-19 disease
At the time of the analysis of Study 2, information presented is based on participants 16 years and older. Participants had been followed for symptomatic COVID-19 disease for at least 2,214 person-years for the COVID-19 mRNA Vaccine and at least 2,222 person-years in the placebo group. There were 8 confirmed COVID-19 cases identified in the COVID-19 mRNA Vaccine group and 162 cases in the placebo group, respectively. In this analysis, compared to placebo, efficacy of COVID-19 mRNA Vaccine BNT162b2 from first COVID-19 occurrence from 7 days after Dose 2 in participants without evidence of prior infection with SARS-CoV-2 was 95.0% (95% credible interval of 90.3% to
97.6%). In participants 65 years of age and older and 75 years of age and older without evidence of prior infections with SARS-CoV-2, efficacy of COVID-19 mRNA Vaccine BNT162b2 was 94.7% (two-sided 95% confidence interval of 66.7% to 99.9%) and 100% (two-sided 95% confidence interval of -13.1% to 100.0%) respectively.
In a separate analysis, compared to placebo, efficacy of COVID-19 mRNA Vaccine from first COVID-19 occurrence from 7 days after Dose 2 in participants with or without evidence of prior infection with SARS-CoV-2 was 94.6% (95% credible interval of 89.9% to 97.3%).
There were no meaningful clinical differences in overall vaccine efficacy in participants who were at risk of severe COVID-19 disease including those with one or more comorbidities that increase the risk of severe COVID-19 disease (e.g. asthma, BMI ≥ 30 kg/m2, chronic pulmonary disease, diabetes mellitus, hypertension).
Confirmed cases were determined by Reverse Transcription-Polymerase Chain Reaction (RT-PCR) and at least 1 symptom consistent with COVID-19 disease*.
*Case definition (at least 1 of): fever, new or increased cough, new or increased shortness of breath; chills, new or increased muscle pain, new loss of taste or smell, sore throat, diarrhoea or vomiting.
5.2 Pharmacokinetic properties
Not applicable.
5.3 Preclinical safety data
Non-clinical data reveal no special hazard for humans based on a conventional study of repeat dose toxicity. Animal studies into potential toxicity to reproduction and development have not been completed.
6. PHARMACEUTICAL PARTICULARS
6.1 List of excipients
ALC-0315 = (4-hydroxybutyl) azanediyl)bis (hexane-6,1-diyl)bis(2-hexyldecanoate),
ALC-0159 = 2-[(polyethylene glycol)-2000]-N,N-ditetradecylacetamide,
1,2-Distearoyl-sn-glycero-3-phosphocholine,
cholesterol,
potassium chloride,
potassium dihydrogen phosphate,
sodium chloride,
disodium hydrogen phosphate dihydrate,
sucrose,
water for injections
6.2 Incompatibilities
In the absence of compatibility studies, this medicinal product must not be mixed with other medicinal products.
6.3 Shelf life
6 months at -80 °C to -60 °C.
6.4 Special precautions for storage
Store in a freezer at -80 °C to -60 °C.
Store in the thermal container at -90 ºC to -60 ºC.
Store in the original package in order to protect from light.
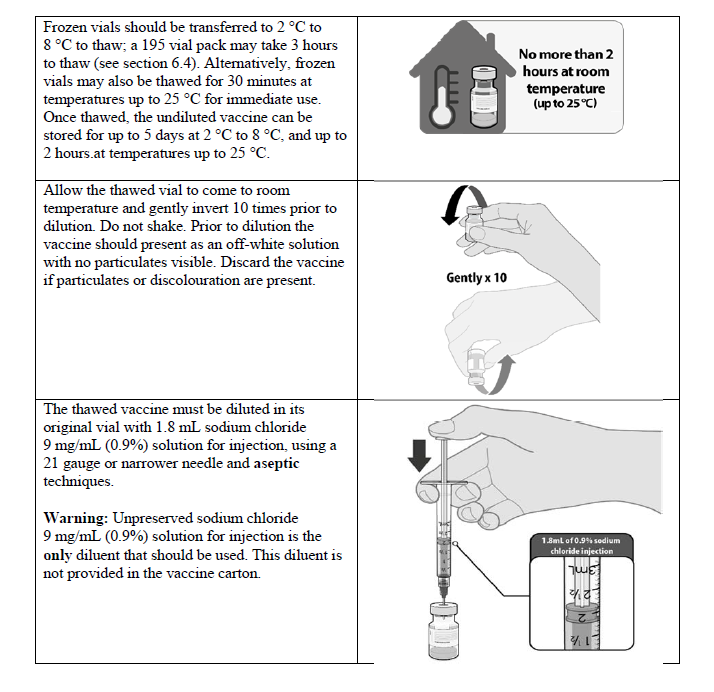
After thawing, the vaccine should be diluted and used immediately. However, in-use stability data have demonstrated that once thawed, the undiluted vaccine can be stored for up to 5 days at 2 °C to 8 °C, or up to 2 hours at temperatures up to 25 °C, prior to use. During storage, minimise exposure to room light, and avoid exposure to direct sunlight and ultraviolet light. Thawed vials can be handled in
room light conditions.
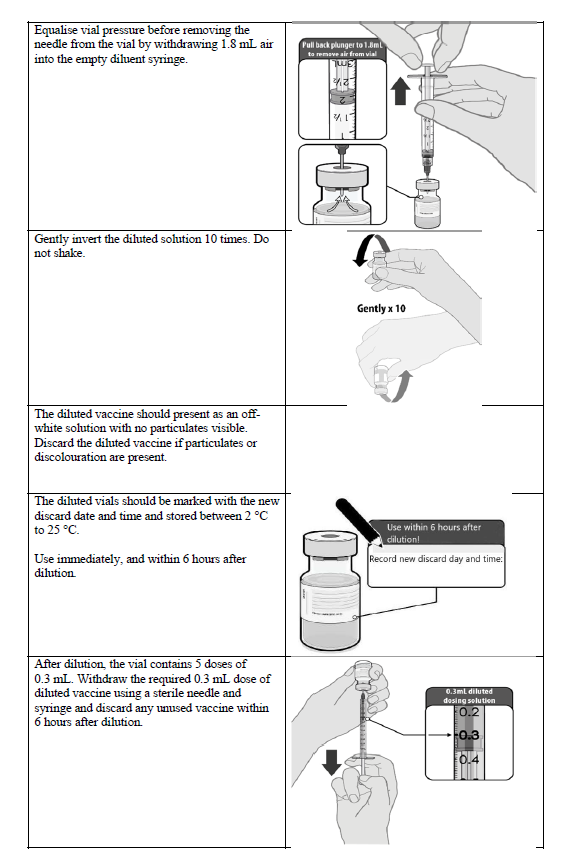
After dilution, store the vaccine at 2 °C to 25 °C and use immediately and within 6 hours. The vaccine does not contain a preservative. Discard any unused vaccine. Once diluted, the vials should be marked with the new discard date and time. Once thawed, the
vaccine cannot be re-frozen.
6.5 Nature and contents of container
Concentrate for solution for injection for 5 doses in a 2 mL clear vial (type I glass) with a stopper (bromobutyl) and a flip-off plastic cap with aluminium seal.
Pack size: 195 vials
6.6 Special precautions for disposal and other handling
Any unused medicinal product or waste material should be disposed of in accordance with local requirements. For instructions on dose preparation of the medicinal product before administration, see section 4.2.
7. MARKETING AUTHORISATION HOLDER
Not applicable.
8. MARKETING AUTHORISATION NUMBER(S)
Not applicable.
9. DATE OF FIRST AUTHORISATION/RENEWAL OF THE AUTHORISATION
Not applicable.